
The Connection Pathway
How Clinical Medicine Informs Longitudinal Member Engagement

Summary
In medicine, the path to lasting outcomes is a coordinated, evidence-based sequence of care designed around a patient’s journey. Clinical pathways help transform healthcare by mapping the right action with the right need at the right moment. Associations can apply these lessons to how we design for durable belonging.
This is an article about connection pathways: a structured, collaborative approach to building trust, contribution, and community that creates healthy rhythms and lasting member loyalty. They are contagions for progress and anchors for new revenue.
I lead the product community, a product development learning community designed specifically for associations. Let’s compare ideas and build something great.
What We Can Learn From Medicine
“The goal of the clinical pathway is to bring the best evidence to the bedside every time, for every patient.”
Leigh Kinsman
Forty years ago, healthcare faced a problem. The same diagnosis produced wildly different outcomes depending on who was on call. Triggered by a lack of alignment, costs ballooned and patients received inconsistent care.
Clinical pathways helped solve the problem. Defined as a structured multidisciplinary care plan that translates clinical guidelines into sequenced action, it gave every member of the care team (physicians, nurses, pharmacists, rehab specialists) a shared map. The pathway provided the architecture within which judgment could be exercised coherently. Pathway-guided care resulted in shorter hospital stays, fewer complications, and lower costs. Collaboration and coordination won the day.
In healthcare, guidelines tell clinicians what should be done. Clinical pathways specify when, where, and how translated into the culture of a specific institution and specific patient population. In associations, our strategic plans define engagement. Our through line is anchored by connection pathways: a sequenced, collaborative, member-centered system that focuses on durable connection, ongoing guidance, and high impact outcomes.
A Cumulative Journey
“Confidence will feel less like a mask and more like muscle memory. If you are new and unsteady, you are not behind. You are at the start of the only path that lasts. Build the map. Honor the risks.”
Alvis Ng
Authentic member needs rarely align with our renewal cycle, annual conference, or content calendar. Deep connection is a product of accumulated, sequenced experience over time: trust built in layers, contribution invited at the right career moment, community formed around shared challenge rather than shared geography.
In medicine, this is called usual care: each encounter is treated independently with providers acting from separate protocols. Similar to the standard association experience, the patient experience is fragmented. Members join, attend a conference, take a course, consume content. If no one is responsible for the sequence (from first touch to deep belonging) then we operate from a portfolio of interventions, not a system of aligned care. This episodic model produces inconsistent value and spotty loyalty.
A connection pathway changes the logic. It is a structured, evidence-informed sequence of experiences designed across functions, mapped to career moments, and governed by clear progression criteria. The purpose is to transform a new member into a deeply connected contributor. Drawn from clinical pathway design, several defining characteristics emerge:
Aspiration translates to action. Our strategic plans promise purpose aligned to community. A connection pathway specifies how it works for diverse member segments: a young professional in their first leadership role, a mid-career practitioner navigating a pivot, a veteran preparing to give back. The pathway tells us what to do, in what order, and who guides each step.
Practice is multidisciplinary. A clinical pathway works because it aligns the care team; no single role carries the whole load. Connection pathways are similar. Membership, education, community, and communications each play a defined function in the sequence. The pathway makes these handoffs explicit. When a member completes their first learning experience, who reaches out and why? When a member indicates interest, who invites them into a contribution role?
Progress is criteria-based. Clinical pathways advance based on patient progress: clinical indicators, readiness markers, response to treatment. Connection pathways should function the same way. A member who has attended three events, taken one course, and participated in two community discussions is not the same as a member who has done none of those things. Pathway progression is triggered by demonstrated engagement and readiness.
Personalize for the masses. Clinical pathways are designed for the majority of cases, preserving clinician judgment for outliers. Well-designed connection pathways should work similarly. We build bespoke experiences for hypothetical members and struggle to scale or replicate them. A connection pathway creates reliable structure for the most common member journey, while leaving room to exercise judgment when members’ needs diverge.
Clinical pathways are evaluated against defined outcome criteria: complication rates, length of stay, readmission. Connection pathways should be no different, yet also measure for deeper engagement. What are the equivalent indicators? Progression from consumption to contribution, depth of peer network formed, self-reported sense of belonging at 12 and 24 months, engagement across multiple touch points rather than a single program. These outcomes happen when we design for them.
The Three Stages of the Connection Pathway
“When people can see the steps ahead, they’re more engaged, motivated, and committed. Development pathways send a powerful message: your growth matters here. They map careers, roadmaps, build confidence, and provide autonomy.”
Jessica Oppenheim
In my earlier work on learning pathways, I described a three-stage arc: pre-learning, knowledge gain, and application / giving back. A connection pathway is similar, but the currency is trust and belonging rather than content and skill.
Stage One: Orientation and Trust-Building
The clinical pathway equivalent is the initial assessment and stabilization phase. For a new member, this is when they decide whether the association is worth their time, identity, and attention. Intentionality is key. Onboarding is a coordinated set of experiences designed to anticipate a new member’s most urgent unspoken questions: Do I belong here? Does this community foster openness and honesty? Do they understand the problems I’m trying to solve?
Trust is built through encounter, through moments of genuine recognition, peer engagement, and psychological safety. This stage is less about content and more about connection infrastructure: mentor pairings, cohort introductions, and facilitated conversations that reveal shared, professional interest.
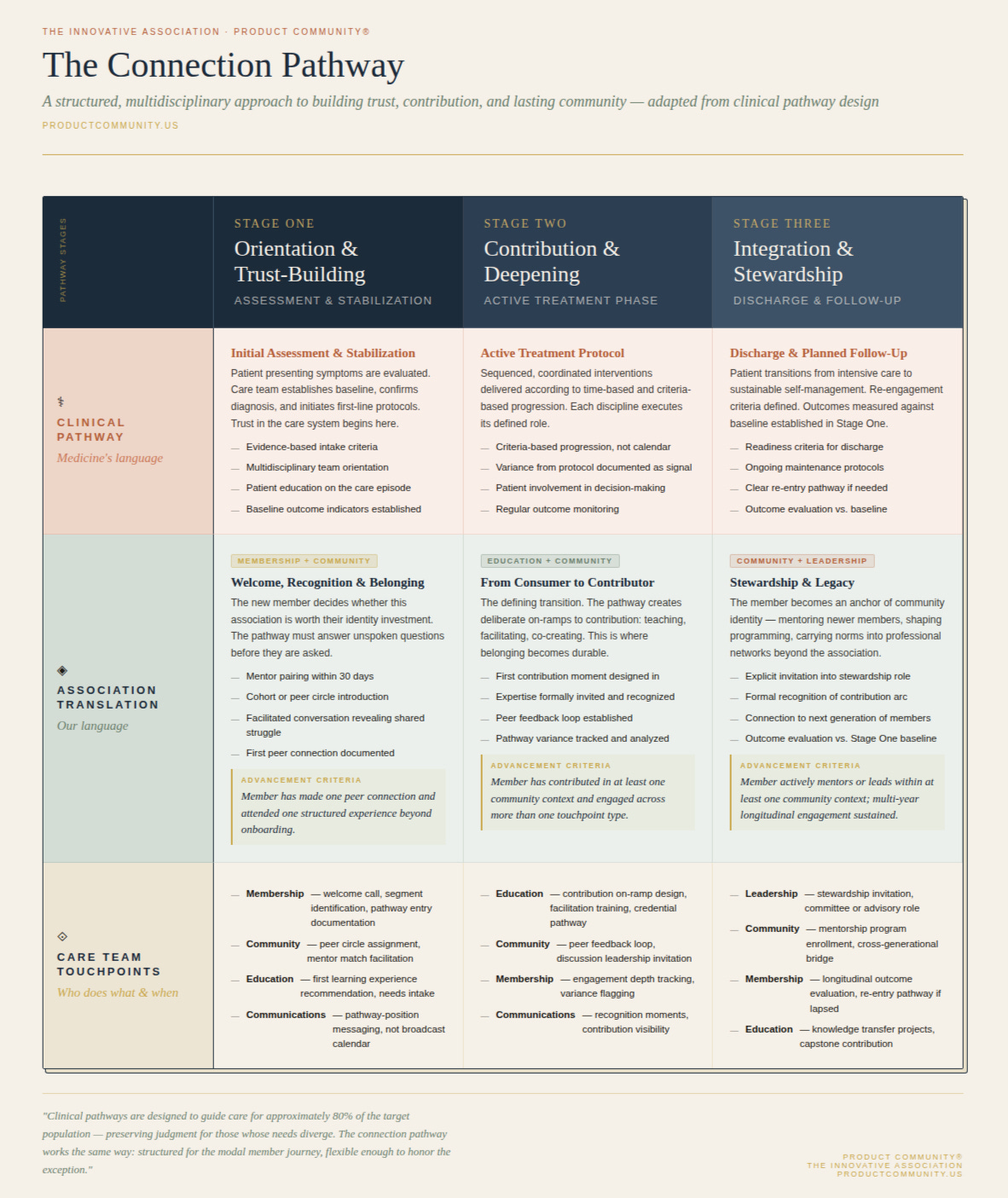
Stage Two: Contribution and Deepening
In clinical care, this is the active treatment phase, where protocol guides the sequenced application of evidence-based interventions. It is where progress is monitored against defined indicators. In a connection pathway, this is when a member moves from received benefits to active participant. A pathway should create deliberate on-ramps to contribution: sharing a perspective in a community forum, co-facilitating a discussion, or the first time one’s expertise is formally recognized.
This stage can be a struggle for associations. We invest in member acquisition and retention, but under-invest in the transition from passive consumer to active contributor which is the defining shift toward lasting connection. Contribution is a therapeutic intervention. It deepens stakes in the community, builds identity, and creates the relational bonds that outlast any single program.
Stage Three: Integration and Stewardship
Clinical pathways include discharge and follow-up. This is the planned transition from intensive care to ongoing maintenance with criteria for as-needed re-engagement. For connection pathways, this is a member’s full integration into the community as active steward. They mentor newer members, shape programming, and carry the community’s norms and values into their professional networks.
This is the decade-four and decade-five professional from the member journey map. They are the wisdom-keeper and standard-setter. The pathway continues to matter. Integration is not spontaneous. It requires an explicit invitation into stewardship roles, formal recognition of contribution, and continued connection to the next generation of members whose own pathways they now help to anchor.
Association as Coordinated Care Team
Clinical pathways force a re-thinking of organizational structure. They demand defined roles and trusting collaboration to foster coordinated care as an aligned team. In medicine, the pathway assigns specific responsibilities to the physician, nurse, pharmacist, and physical therapist at each stage of care. No one does everything; everyone has a role. The result is fewer gaps, fewer redundancies, and far better patient outcomes.
How would this look like in an association? Membership knows the entry criteria and guides the first-stage welcome. Education designs the contribution on-ramps in stage two. Staff responsible for community own peer network formation and the transition to durable contributor. Communications delivers the right signal at the right moment. Leadership owns the stewardship invitations.
Success comes from alignment, discipline, and trust. The pathway is the shared map that makes cross-functional ownership possible. This shared ownership drives predictable rhythms that foster member confidence.
Clinical pathway researchers track variance or deviation from the expected pathway sequence. When a patient progresses faster or slower than anticipated or when the team deviates from the protocol, the variance is documented, analyzed, and treated as a signal. This feedback loop is an opportunity for associations. We launch programs and measure attendance. We track renewals and measure net promoter scores. But we need to ask: Where did members deviate from the expected engagement sequence? What did we learn? How did we adjust? How would we plot members in this engagement diagnostic?
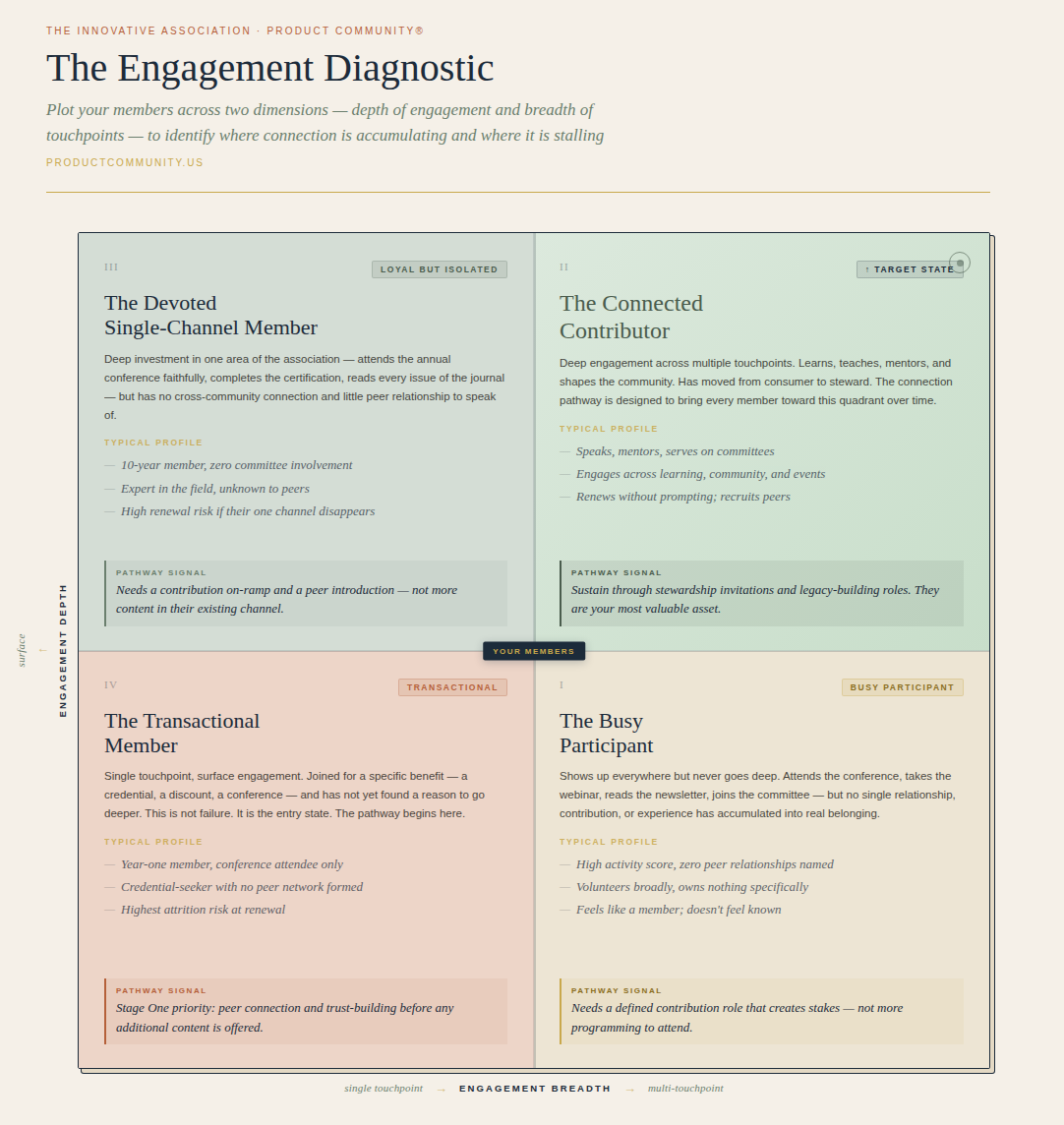
Variance in a connection pathway provides valuable data. The member who dropped out between stage one and stage two tells us something about our trust-building infrastructure. A member who accelerated through stage two and arrived at stage three without a formal invitation tells us something about under-built contribution on-ramps. A commitment to pathway variance turns a member engagement system into a self-improving learning system.
This is what I call compound value. A well-designed connection pathway generates the data and institutional learning that improves year two and makes year three better still. Well-designed and implemented, a pathway appreciates with use. While clinical pathway skeptics argue that structured protocols reduce clinicians to technicians (fostering cookbook medicine that strips professional judgment and human nuance), they can leave room for improved judgment because the structural burden is lifted and attention shifts to genuine, patient-centric care.
The same is true for associations. Deployed transactionally, connection pathways become depersonalized scripts, a way of automating our human instincts. A predictable structure shouldn’t replace a mentor’s wisdom or a community manager’s outreach. It gives those qualities a stage to perform. It ensures that human encounters happen in the right way at the right moment.
Structure and belonging are complements. Members trust systems they can predict and invest in coherent journeys. Repeatability anchors human connection.
Building Your First Connection Pathway
“What feels like play to you, but looks like work to others? That’s your path to leverage.”
Naval Ravikant
Clinical pathways are built for high-volume, high-stakes diagnoses where structured coordination produces the clearest return. In associations, we start with our most critical member segment and most important transition: the journey from new member to first contribution. Map the existing touch points, identify who owns each one, and name the gaps where no one is responsible. Define three to five criteria that tells you a member is ready to advance from trust-building to active contribution.
Then ask the harder question: Who is the care team? Who is responsible for this member’s journey at each stage and what do they specifically do?
The answers reveal misalignment by surfacing missed handoffs, single-use one and done programming, and the contribution on-ramps that only exist in theory. These gaps are the beginning of our connection pathway.

Clinical pathways changed medical outcomes. Outcomes used to be something that happened to patients, now they are something care teams design for. Connection pathways ask us to make the same shift. We design for belonging with intentionality, coordination, evidence, and a commitment to learning from people and data. The member who trusts, contributes, and stays is both a participant and product of pathway design.
Associations are the de facto partners in our members’ career-long journeys. Clinical pathways remind us that durable outcomes require more than good intentions and good content. They require coordinated, sequenced, member-centered design delivered consistently, evaluated honestly, and improved continuously.
That is the connection pathway. Get started today.
I lead the product community; we are a learning community because we believe great relationships help us create the value our members want. Remember, product-led growth fuels connection. Join the product community and flip your destiny.
About the Author
James Young is founder and chief learning officer of product community®. Jim is an engaging trainer and leading thinker in the worlds of associations, learning communities, and product development. Prior to starting product community®, Jim served as Chief Learning Officer at both the American College of Chest Physicians and the Society of College and University Planning. Please contact me for a conversation: james@productcommunity.us